2.1.Overview of Module 2
This module provides an overview of recommended dietary intakes and factors that affect vitamin C intake and body status, and outlines the different tools and methods used to measure dietary vitamin C intake and concentrations of the vitamin in biological samples. This Module also contains a number of practical activities for you to explore these methods. The module also outlines the different types of studies used to assess vitamin C status and efficacy.
Following completion of this module the participant will be able to:
- Demonstrate understanding of factors that affect vitamin C intake and body status and communicate this with their patients (Communication, Scholarship, Professionalism)
- Discuss how to assess and improve dietary vitamin C intake with their patients (Communication, Scholarship, Professionalism)
- Apply knowledge on vitamin C assessment to their healthcare practice (Clinical expertise, Professionalism)
- Demonstrate awareness of the different study designs used to assess vitamin C and the strengths of their evidence (Scholarship, Professionalism)
Length of activity: 90 min (20 min reading + 70 min activities)
RNZCGP Endorsed: 1.5 CME credits
CICM Accredited: 1.5 points
2.2. Dietary vitamin C intake
As you learnt in Module 1, dietary vitamin C is synthesised in plants and the livers (or kidneys) of most animals – other than humans and a handful of other animal species – due to random genetic mutations that have 'knocked out' a key enzyme in the biosynthetic pathway. As such, we obtain vitamin C primarily from fresh fruit and vegetables in our diet. Some cultures (e.g. Inuit) also obtain vitamin C from animal livers, but this is less common in modern Western societies. Because vitamin C is water-soluble, it is not stored in the body (like the fat-soluble vitamins are) so it needs to be consumed on a daily basis to maintain optimal levels in the body.
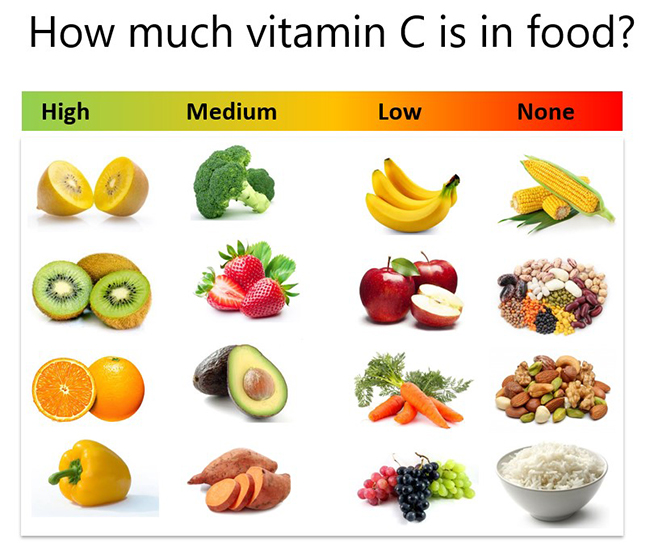
Something we need to keep in mind, however, is that not all fruit and vegetables are created equal when it comes to their vitamin C content. Some fruit such as citrus fruit, kiwifruit and guava are quite high in vitamin C, however, other commonly consumed foods such as bananas and apples are actually quite low in vitamin C (see figure below). Therefore, it is important to consume a variety of fruits and vegetables. It is also important to note that most staple foods, such as rice, wheat, millet and corn, contain negligible vitamin C. Furthermore, animal products, such as most meat (other than liver), eggs, and milk also contain negligible vitamin C.
The vitamin C content of food can also be affected by a number of different factors, such as time of harvest, transport and storage conditions, and cooking. Because vitamin C is water soluble and heat sensitive, cooking can decrease the vitamin C content of food. Therefore, it is ideal to consume some raw fruit and vegetables each day to make sure you are getting your recommended vitamin C intakes. Because vitamin C is a good antioxidant, it is sometimes added to foods as a preservative, e.g. fruit juices often contain added vitamin C.
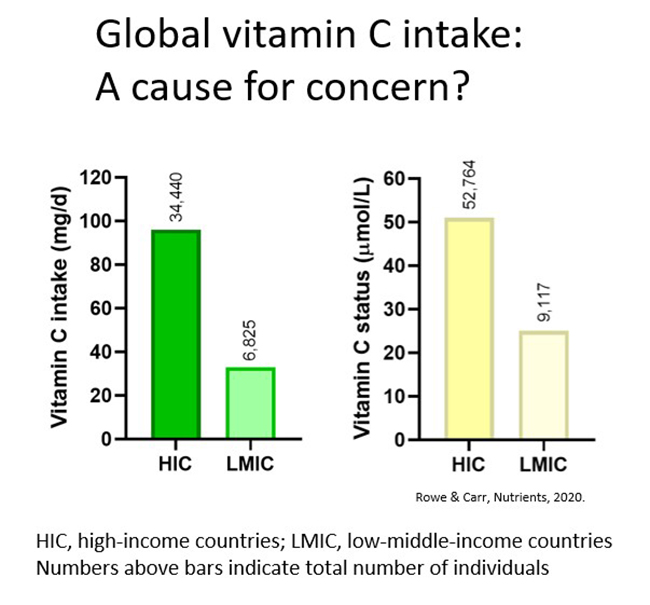
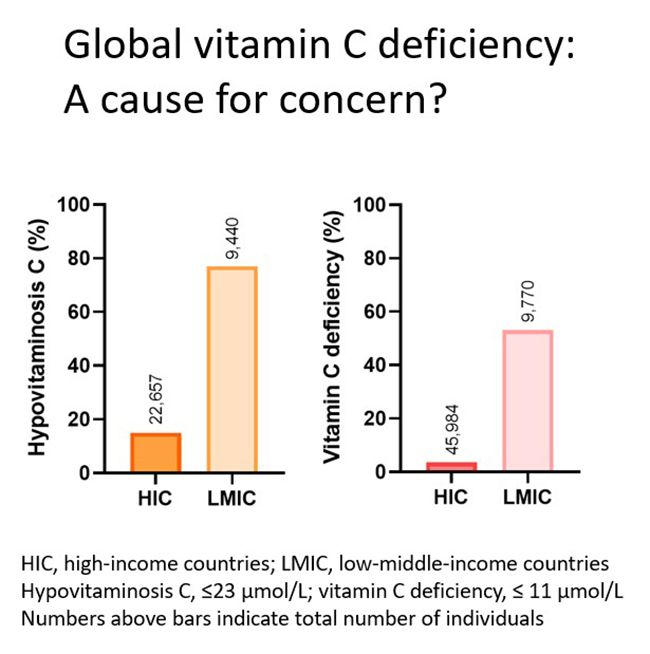
According to the Global Burden of Disease initiative, low fruit and vegetable consumption are two of the top five contributors to global mortality. As Hippocrates (400 BC) stated: Let food be thy medicine and medicine be thy food. Overall, obtaining optimal vitamin C intake through diet is recommended due to the presence of other beneficial micronutrients and phytochemicals. However, this is not always possible for many people due to their circumstances. For example, many low-middle income countries (LMIC) have dietary intakes that comprise primarily of staple foods with minimal high vitamin C fruit and vegetables. This can contributes to those populations having low vitamin C status (see figure below).
2.2.1. Activity: High vitamin C foods
Timing: 5 min
Open up or print off the below resource. Make a note of or highlight the different types of fruit and vegetables that you typically consume as part of your diet. How many of these are high vitamin C foods?
If you do not consume many high vitamin C foods, do you think you could incorporate more vitamin C rich foods into your diet? If so, note or highlight these on your list and over the next week make an effort to consume more of these foods in your daily diet.
2.3. Recommended vitamin C intakes
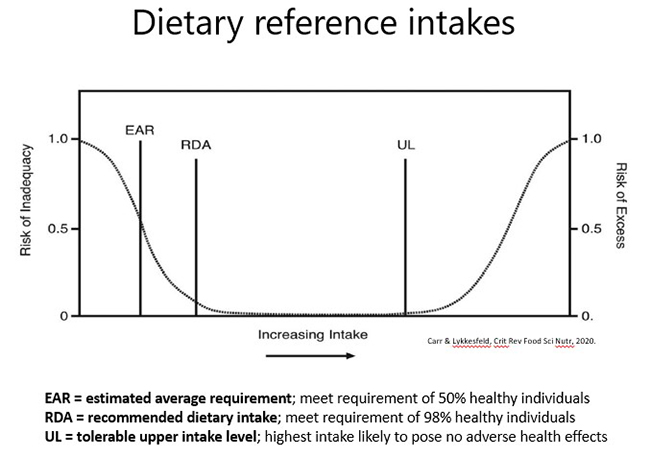
During World War II recommended dietary allowance (RDA) criteria were established in order to identify nutritional issues that might affect national defense. As such, RDAs were initially set at intakes that would prevent outright deficiency disease (with a margin of error) in 97.5% of healthy individuals (see figure below). In the case of the vitamin C deficiency disease scurvy, intakes of vitamin C as low as 10 mg/day will prevent the overt signs and symptoms of the disease. Therefore, vitamin C RDAs were initially set as low as 30 mg/day and, today, some authorities (e.g. WHO) and regions of the world (e.g. the UK, AUS/NZ) still have RDAs that are not much higher than this (i.e. 40-45 mg/day).
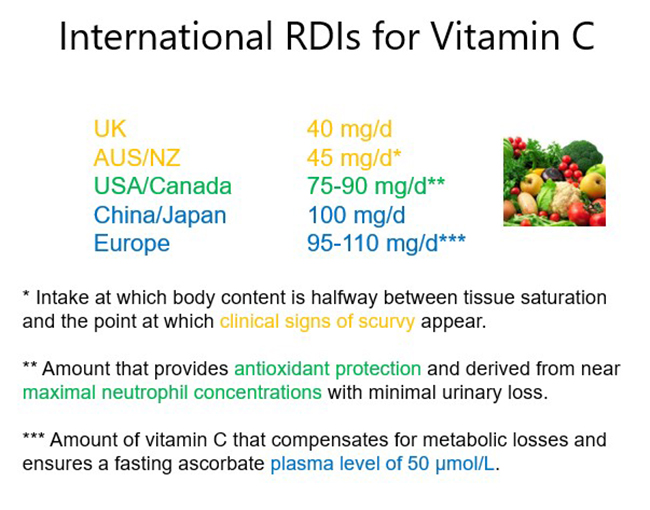
Numerous countries have updated their RDAs (also known as dietary reference intakes/values [DRIs/DRVs], reference nutrient intakes/values [RNIs/RNVs], recommended dietary intakes [RDIs], etc, depending on the country) and now have RDAs that are based on the potential health effects of vitamin C or on vitamin C pharmacokinetics. As such these values are higher, typically around 100 mg/day vitamin C (see figure below). Some countries (e.g. China, AUS/NZ) also have a proposed intake (PI) or suggested dietary target (SDT) for the reduction of chronic disease risk of ~200 mg/day vitamin C. As you learnt in Module 1, an intake of 200 mg/day vitamin C will provide saturating plasma status in healthy people.
Because vitamin C is water-soluble, and any excess that the body does not need is readily excreted in the urine, there is no upper limit for toxicity. This was discussed in Module 1 under safety. However, some countries have set 1-2 g/day as an upper limit to eliminate any possibility of gastrointestinal disturbance from unabsorbed vitamin C that can occur in some people at doses >4 g/day.
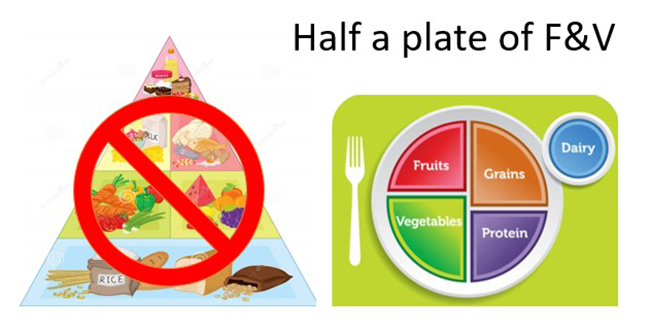
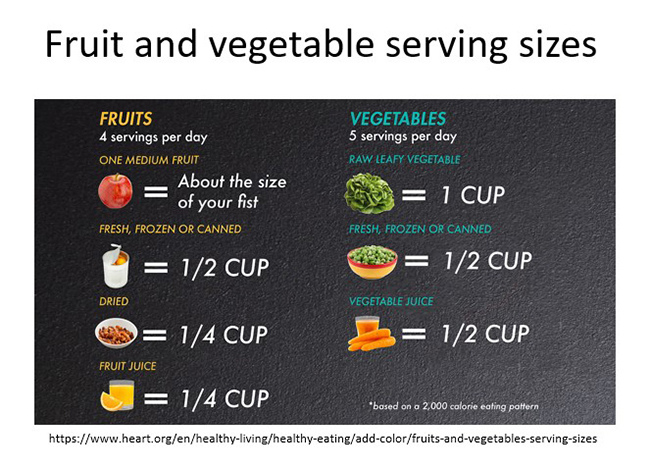
A dietary intake of 200 mg/day vitamin C can be obtained from consuming 5+ servings of fresh fruits and vegetables per day, as long as at least one serving is a high vitamin C food. Recommendations are for a higher ratio of vegetables to fruit if possible e.g. 3 vegetables and 2 fruit. Some countries (e.g. the USA/Canada) recommend a diet of 7-9 servings of fresh fruit and vegetables per day. The old 'food pyramid', which used to comprise grains as the largest food group, has now been replaced by the plate system whereby fruits and vegetables should comprise half of each plate full of food that you consume (and grains and protein only one quarter each).
Further reading:
- Discrepancies in global vitamin C recommendations: a review of RDA criteria and underlying health perspectives. Carr and Lykkesfeldt, Nutrients, 2020.
This recent review highlights the different global RDAs for vitamin C and critiques the criteria used to establish these. - Toward a new recommended dietary allowance for vitamin C based on antioxidant and health effects in humans. Carr and Frei, Am J Clin Nutr, 1999.
This review highlights the potential antioxidant effects of vitamin C in various health conditions and helped inform the last update of the US RDA for vitamin C (RDA was increased in the year 2000).
2.3.1.Activity: Half a plate
Timing: 5 min per day over 1 week (35 min total)
Every time you consume a meal over the next 3 days – look down at your plate and estimate what proportion of it comprises fruit and vegetables vs grains and protein. Note this down.
If you are consuming less than half a plate of fruit and vegetables with each meal, over the following 3 days, try and increase the proportion of fruit and vegetables on your meal plates. Note this down.
On the seventh day compare these notes with those from your first 3-day phase and ask yourself the following questions:
- Have you been able to increase your fruit and vegetable consumption? By how much?
- Did you changing your diet influence those around you e.g. those living in the same household?
- Is there still room for improvement? If yes, how might you achieve this?
2.4.Supplemental vitamin C
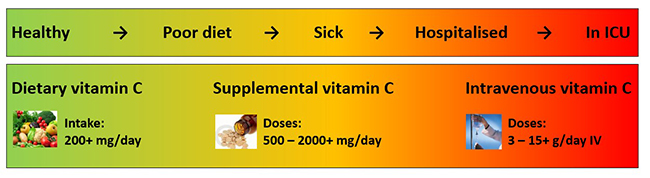
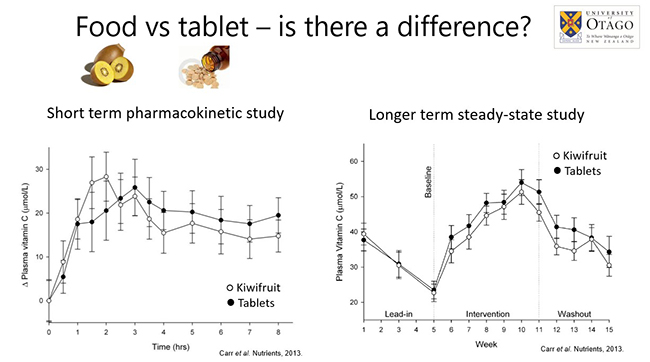
If a healthy person is consuming a diet of at least 5+ servings of fresh fruits and vegetables per day, and at least one of those servings is a high vitamin C food, then they should be able to get their optimal vitamin C intake (200 mg/day) through diet alone. However, US data (2015) indicates that only 1 in every 10 American is meeting their fruit and vegetable recommendations and in Canada, only 20 percent of women and 11 percent of men hit their daily target. Note that the bioavailability of vitamin C from food sources is equivalent to that from tablets in humans, i.e. other components in foods do not affect the uptake of vitamin C (see figures below). If a person has a poor diet, for whatever reason, they will likely need to supplement in addition to their daily diet (see figure below). If a person comes down with an acute illness (e.g. an infection) or has an ongoing chronic condition (e.g. cancer), their vitamin C requirements will increase and they may need intravenous vitamin C. This will be discussed in more detail in subsequent modules.
Research has indicated that the bioavailability of vitamin C from tablets is equivalent to that from food sources in humans, i.e. other components in foods, e.g. bioflavonoids, do not affect the uptake of vitamin C (see figures below). Many different supplement formulations are commercially available (e.g. powder, capsules, tablets, chewable, slow release), however, because the body is very good at absorbing ingested vitamin C regardless of the source, they all appear to provide fairly comparable vitamin C uptake (see further reading below). Although it has been proposed that liposomal vitamin C provides superior uptake (liposomes are taken up by different mechanisms to the normal intestinal vitamin C transporters SVCT1), the evidence for additional health benefit is currently lacking.
Further reading:
- Synthetic or food-derived vitamin C - are they equally bioavailable? Carr and Vissers, Nutrients, 2013.
This review covers the evidence around the comparative bioavailability of food-derived and synthetic vitamin C
2.5.Assessment of dietary vitamin C intake
Dietary intakes of vitamin C can be estimated using a variety of tools.
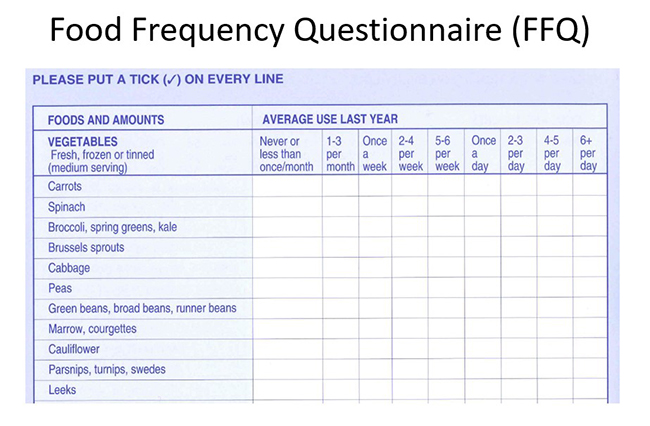
Food frequency questionnaire (FFQ)
The most commonly used is a 'food frequency questionnaire' which tracks what people have been eating over a certain period of time (usually 6 month or a year – see an example below). As you can imagine, these are relatively rough estimates of an individual's dietary intake and can be prone to reporter bias.
24-hour dietary recall
Another tool is called a '24-hour dietary recall', whereby everything a person has consumed over the previous 24 hours is recorded. However, as you can imagine, intakes can vary significantly depending on the day of the week. Therefore, several recalls, on different days of the week are preferred. Also, dietary intakes will vary depending on the time of the year (season).
Daily food diary
Finally, a daily food diary, whereby the person records everything they consume (foods and drinks) over usually a 7-day period is generally the most accurate. Furthermore, in order to determine the vitamin C content of the foods and beverages consumed, the exact amounts and how they were prepared also need to be recorded. The servings of fruit and vegetables can be estimated from their size or household measures or metric weight/volume. However, in order to calculate the vitamin C content consumed, specialist expertise and software is required. Nutrition or dietetic graduate students are often available to do this if required.
2.5.1.Activity: 24-hour food diary
Timing: 10 min per day over 3 days (30 min total)
Pick a week day and record everything you eat and drink on that day (breakfast, lunch, dinner and snacks). Pay particular attention to your fruit and vegetable intake, including juices/smoothies and mixed meals that may contain some fruit and/or vegetables as components.
You can record your intake in a notebook, on your phone or using the resource template (below) – either at the time or at the end of the day (you could also take photos of each meal).
Note: it is important to record how much or the size of each item you consume using household measures or metric volumes/weights (see examples in the resource or the figure below).
Then pick a weekend day and do the same thing – record everything you consume, including amounts. Do you eat different things on weekdays vs weekends?
On the third day, see if you can estimate how many servings of fruit and vegetables you consumed on each of those days. The size of typical fruit and vegetable servings are shown below.
Are you consuming at least 5+ servings of fruit and vegetables per day? If not, can you think of ways to incorporate more fruit and vegetables into your daily diet (ideally 7-9 servings)?
2.6.Factors that can affect body vitamin C status
There are a number of factors that can affect body vitamin C status.
Dietary intake
The primary factor is dietary intake (as discussed above). Global studies indicate that populations with low socioeconomic status/higher deprivation, including those from low-middle income countries, have a higher proportion of hypovitaminosis C (≤23 µmol/L vitamin C) and outright deficiency (≤11 µmol/L vitamin C) (see figures below). Large epidemiological studies have indicated that vitamin C deficiency is not observed in people who supplement.
Pollution and cigarette smoke
Because vitamin C is a potent antioxidant, the oxidants present in air pollution and cigarette smoke, including passive smoking, can deplete the body stores of the vitamin. Epidemiological research (including NHANES, the Canadian Health Measures Survey, EPIC-Norfolk, and the French POLA study and SU.VI.MAX study baseline) have indicated that smokers have lower vitamin C status and a higher prevalence of deficiency relative to non-smokers. Some authorities have taken this into consideration with higher vitamin C recommendations for smokers comprising additional intakes of 20 to 80 mg/d over the RDA for adults in these countries.
Health factors
Many acute and chronic disease states are also associated with enhanced oxidative stress and inflammation, both of which are associated with lower vitamin C status, independent of dietary intake. Higher body weight is also associated with lower vitamin C status, which could be due to the enhanced oxidative stress and inflammation observed in obesity, but is also likely due to a volumetric dilution effect. Health factors that affect vitamin C status will be discussed in more detail in subsequent Modules.
Further reading:
- Global vitamin C status and prevalence of deficiency: A cause for concern? Rowe and Carr, Nutrients, 2020.
- Factors affecting vitamin C status and prevalence of deficiency: A global health perspective. Carr and Rowe, Nutrients, 2020.
These two comprehensive reviews explore the vitamin C status of populations from different countries and the various factors that affect vitamin C status globally.
2.7. Measurement of vitamin C in biological samples
2.7.1.Sample acquisition and handling
Plasma (or serum): is the most commonly used medium for measuring body vitamin status due to ease of access. Because vitamin C intake results in a peak in plasma concentrations approx. 2 hours following ingestion (in healthy people), recent dietary intake can dramatically affect plasma vitamin C concentrations. As such, fasting plasma concentrations are preferred. This is less of an issue in people who have hypovitaminosis C or outright deficiency as any recent vitamin C intake is not likely to affect their blood levels due to rapid uptake of the vitamin by depleted tissues.
Leukocytes: are thought to better reflect body vitamin C status and are relatively easy to isolate from blood. Leukocyte subtypes can contain different vitamin C concentrations. Furthermore, these cells can also uptake additional vitamin C following activation due to oxidation of extracellular vitamin C to dehydroascorbic acid which is readily transported through their membrane glucose transporters (GLUT) and subsequently reduced back to vitamin C intracellularly.
Tissue biopsies: have also been used to assess vitamin C status, however, they are an invasive procedure and vitamin C concentrations vary in different tissues depending on their requirements for vitamin C, e.g. muscle tissue has relatively low concentrations of vitamin C.
Urine: excretion of vitamin C can be assessed in urine samples and peaks about 3 hours following ingestion (in healthy people). Spot samples should be standardised to urinary creatinine to account for dilution. Ideally 24-hour collections should be carried out, but this is not always possible.
Due to the instability of vitamin C once removed from the body, careful handling, processing and analysis of biological samples is required to prevent its oxidation and obtain accurate results. Vitamin C is relatively unstable in plasma (particularly EDTA plasma – see further reading below), and requires either immediate analysis or freezing at -80°C for short term storage. Ideally, the samples are acidified and a metal chelating reagent added to aid in stabilisation for longer term storage at -80°C. Vitamin C can be measured in cells and tissues following lysis or homogenisation of the samples and processing as for plasma.
Further reading
- Appropriate handling, processing and analysis of blood samples is essential to avoid oxidation of Vitamin C to dehydroascorbic acid. Pullar et al. Antioxidants, 2018.
This research paper highlights the lack of oxidised vitamin C (DHA) in different patient samples and critiques the methodologies which can lead to artifactual/ex vivo oxidation. - Principles of Nutritional Assessment: Vitamin C. Carr A, in Principles of Nutrition Assessment, 2022 (3rd edition).
This online book chapter discusses the indices of vitamin C status with regard to nutritional assessment.
2.7.2.Analytical methodologies and equipment
Spectrophotometric methods: There are a number of colourimetric or fluorimetric 'test-tube' assays which utilise chemical reactions between chromophores or fluorophores and the oxidised form of vitamin C (i.e. vitamin C has to first be oxidised to dehydroascorbic acid). However, these are not specific for dehydroascorbic acid and are therefore prone to interference by other compounds in the samples and are also prone to artifactually higher levels of dehydroascorbic acid in the 'unoxidised' samples.
 High performance liquid chromatography (HPLC): The gold standard method for measuring vitamin C in biological samples is high performance liquid chromatography (HPLC) with either electrochemical or UV detection. This method is very sensitive and highly specific as interfering compounds are separated out using a column prior to detection. However, this is expensive and technically demanding methodology and is currently not readily available to most healthcare providers.
High performance liquid chromatography (HPLC): The gold standard method for measuring vitamin C in biological samples is high performance liquid chromatography (HPLC) with either electrochemical or UV detection. This method is very sensitive and highly specific as interfering compounds are separated out using a column prior to detection. However, this is expensive and technically demanding methodology and is currently not readily available to most healthcare providers.
Urine test strips: are available to detect vitamin C excreted in urine. However, there is a non-linear relationship between plasma and urine vitamin C levels, as vitamin C excretion only increases significantly when blood levels reach saturation, so the test strips are indicative of saturation versus non-saturation.
Point-of-care devices: There are currently point-of-care devices in development which, if successful, will greatly aid in routine assessment of people's general vitamin C status, with the caveat that these will not be as accurate as HPLC analysis and so will likely only be indicators of sufficiency versus insufficiency.
Further reading:
- Ascorbic acid and dehydroascorbic acid analyses in biological samples. Washko et al. Analyt Biochem, 1992.
Although an older review, this is a comprehensive critique of the different types of methodology that are used to measure vitamin C, from colourimetric assays through to HPLC.
2.7.3. Optional activity: urine vitamin C analysis
Timing: 5 min, four times over a day (20 min total)
If you are happy to purchase some urine vitamin C test strips you can test your urine vitamin C levels. Vitamin C test strips can be purchased at relatively low cost from here. Some multipurpose urine analysis test strips also measure vitamin C, such as these.
Before your first meal of the day measure your urine vitamin C levels using a test strip following the manufacturer's instructions. Then consume a vitamin C-poor meal and approx. 3 hours later re-measure your urine vitamin C levels using a test strip (it takes approx. 3 hours for ingested vitamin C to appear in the urine).
Before your next meal of the day measure your urine vitamin C levels using a test strip. Then consume a vitamin C-rich meal or take a vitamin C supplement and approx. 3 hours later re-measure your urine vitamin C levels using a test strip.
- Were you able to detect any change in your urinary vitamin C levels after eating a vitamin C-poor meal?
- Did your urinary vitamin C excretion increase significantly after a vitamin C-rich meal or supplement?
2.8.Hierarchy of evidence in vitamin C research
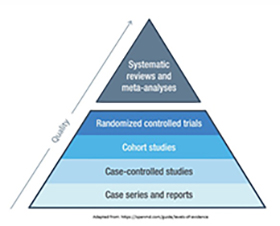 In the following modules you will learn about the roles and uses of vitamin C in different disease states. The progression of evidence in clinical research (sometimes known as the pyramid of evidence – see image below) comprises a number of different study designs, from single case reports or case series, to case control studies, cohort studies, randomised controlled trials, and finally meta-analyses. Some of these have vitamin C-specific caveats which you should be aware of.
In the following modules you will learn about the roles and uses of vitamin C in different disease states. The progression of evidence in clinical research (sometimes known as the pyramid of evidence – see image below) comprises a number of different study designs, from single case reports or case series, to case control studies, cohort studies, randomised controlled trials, and finally meta-analyses. Some of these have vitamin C-specific caveats which you should be aware of.
Single case reports or case series: These are considered to be low quality evidence as there is no control for comparison. In the field of vitamin C research, case reports are generally in relation to cases of scurvy or safety issues, e.g. oxalate nephropathy, G6PD deficiency-related haemolytic anaemia, or point-of-care interference following intervention.
Case control studies: These studies, comprising cases who are compared with controls who have been matched for specific factors (e.g. age, gender, etc), are relatively common in all fields of vitamin C health research. Examples will be given in subsequent Modules, where cases with infection, cancer, and cardiometabolic conditions generally have lower vitamin C levels than matched controls.
Cohort studies: These studies typically follow large numbers of people over long periods of time, sometimes for many years in the case of large epidemiological studies, e.g. NHANES, EPIC-Norfolk study. These can help to determine associations between vitamin C intake or status and specific disease risks or outcomes. Note that these studies can show correlations only and cannot rule out all possible confounding factors or ascertain the direction of causality. Furthermore, vitamin C may simply be acting as a marker of fruit and vegetable consumption, rather than having any biological effects itself (although based on its numerous important physiological roles, it is likely to have an impact on selected outcomes). Longitudinal studies can potentially be used to assess temporal associations e.g. does vitamin C deficiency occur before or after infection or cancer.
Randomised controlled trials: RCTsare considered the 'gold standard' of clinical research as participants are randomly assigned to either a treatment or control group (or act as their own controls in cross-over studies). Although this type of trial paradigm works well for pharmaceutical interventions, it is less suited to vitamin C research for a number of reasons. Firstly, there cannot be a true control group who receives no vitamin C as all the participants will be getting variable amounts through their diets. Also, the participants' baseline vitamin C status (which often isn't assessed) can affect the outcome of the study. For example, if the participant already has adequate vitamin C status at the beginning of the study, then supplementing them with additional vitamin C is unlikely to have much effect on the outcome of interest. If the study is large enough, sometimes sub-group analyses can be carried out e.g. on the people who had deficiency at baseline.
Meta-analyses: These combine data from multiple studies to allow for a larger sample size to provide a better estimate of the treatment effect. These are often used to inform clinical practice. Many meta-analyses have been carried out in numerous fields of vitamin C research, as you will see in upcoming Modules. However, something to keep in mind is that the people who carry out the meta-analyses are not necessarily familiar with the physiology and pharmacology of vitamin C and often combine studies that should not be combined e.g. oral and intravenous studies. This is like combining apples with oranges which will give a non-sensical result (sometimes referred to as 'rubbish in = rubbish out'). Furthermore, although meta-analysis can be carried out with as few as 3 trials, many meta-analyses have been carried out too early, before there are sufficient good-quality trials to warrant them, and in some cases, e.g. vitamin C and sepsis, there are now almost as many meta-analyses as there are primary trials
Further reading:
- On the effect of vitamin C intake on human health: How to (mis)interprete the clinical evidence. Lykkesfeldt J. Redox Biol. 2020.
This comprehensive review highlights the pitfalls of different study design features with regard to vitamin C chemistry and pharmacology.
2.9. Summary of Module 2
- Vitamin C is obtained through the diet, with fruit and vegetables being the primary source, although these can vary significantly in their vitamin C content. Most staple foods (grains) and animal products (meat, eggs, milk) contain negligible vitamin C.
- Recommended dietary intakes for vitamin C vary widely around the world (from 40 to 110 mg/day), with Australia and New Zealand currently having one of the lowest recommendations globally.
- The optimal vitamin C intake is considered to be 200 mg/day, which can be obtained from 5-7 servings of fruit and vegetables per day (as long as at least one serving is high in vitamin C) or aim for 'half your plate'.
- Supplemental vitamin C should be considered if a person has a poor diet or is unwell; most supplemental formulations are fairly comparable in their bioavailability. If a patient is hospitalised or in the ICU, then IV vitamin C administration may be required for repletion of body stores.
- Dietary vitamin C intake can be assessed and monitored using food frequency questionnaires (FFQ), 24-hour dietary recall or daily food diary.
- Dietary vitamin C intake has the biggest impact on plasma concentrations, which is particularly apparent in low-middle income countries. However, other factors such as pollution/smoking and various health factors can affect body stores of the vitamin.
- Vitamin C status can be assessed through measuring fasting plasma or leukocyte concentrations of the vitamin. Urinary excretion can be used as an indirect measure of plasma saturation.
- Vitamin C is relatively unstable in most biological samples so careful handling, processing, storage and analysis is required to prevent its oxidation. Vitamin C concentrations can be quantified by spectrophotometric methods, high-performance liquid chromatography (HPLC; gold-standard method) or urine test strips.
- Various study designs have been used to assess vitamin C status and requirements in different cohorts. Each of these study designs have various pros and cons to be aware of, particularly RCTs (and meta-analyses), which were designed to assess efficacy of drugs, not nutrients like vitamin C.
2.10.Activity: Self-reflection and feedback
Once you have completed all the Modules of interest to you, please complete the self-reflection and feedback form online or email to anitra.carr@otago.ac.nz. For members of the RNZCGP, please include your MCNZ number and the modules completed so that your CPD credits can be uploaded to the RNZCGP website. A certificate of completion can be emailed to you if required.
© Anitra Carr, 2022. You may not copy, modify, distribute, display, transmit, perform, publish or sell any of the copyrightable material on this website. You may hyperlink to this website but must include the following statement: "This link leads to the website 'Oral and intravenous vitamin C use in health care' provided by the Nutrition in Medicine Research Group at University of Otago, Christchurch."